CAH Subcontract Program Application Items
These are the items needed to complete and submit an application to the North Dakota Critical Access Hospital (CAH) Subcontract Program.
CAH Financial/Operational Improvement Area of Choice Application Components
For full consideration, all areas must be completed. Empty spaces could be considered nonresponsive.
 CAH Contact Information
CAH Contact Information
Hospital name, county, address, phone, contact person, email
Select your facility's desired activity to improve finance and/or operations
Only one activity may be selected. Depending on which activity is selected, additional information
specific to the activity is required.
-
Coding and Billing Chart Audit
- Date of facility's last coding and billing audit
- Known or suspected number of coding errors from last audit
- Known or suspected number of missing documentation errors from last audit
-
Chargemaster Review
- Date of facility's last chargemaster review
- Percentage of claim denied
- Clean claims rate
-
Chargemaster Scrub
- Date of facility's last chargemaster scrub
- Known or suspected number of incorrect code errors from last audit
- Known or suspected number of incomplete codes from last audit
-
340B External Audit
- Date of facility's last 340B external audit
- Known or suspected number of duplicate accounts from last external audit
-
Revenue Cycle Management
- Date of facility's last revenue cycle management improvement effort
- Number of registration errors as a percent of total registrations
- Percent of point-of-sale collections
-
Service Line Assessment
- Date of facility's last assessment for the proposed service line
- Average daily census for service line
- Patient utilization of service line
-
Other (For Example: Cost Report Strategy/Compliance Review) Please list current statistics.
- Date of facility's last work related to the proposed activity
- Other metrics that will be considered
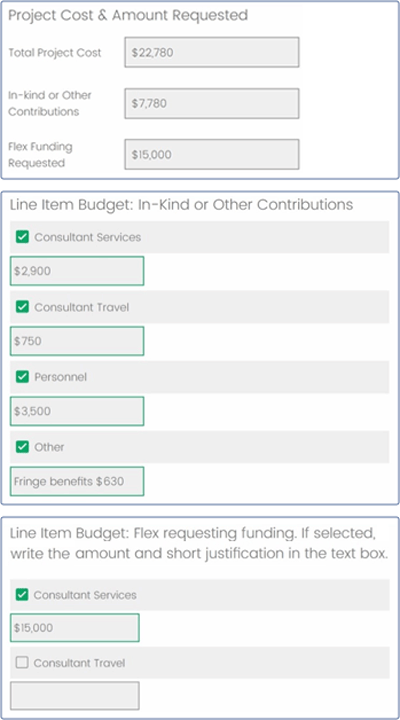
Budget & Budget Narrative – New Process
Enter your project budget and line item details to include information on how the line items are determined
and/or calculated to assist the reviewers in understanding the proposed budget. All budgets should be based
on current vendor quotes. Please note the new budget and budget narrative online format compared to
previous years. Separate budget and budget narrative documents are no longer required to be
uploaded.
Project Management
Name, title, and email of the individual responsible for management and oversight of
this project. Name, title, and email of hospital official authorized to enter into contract.